I’m observing the open/stay home discussions (!) on FB and today’s opening salvo was a picture of an iceberg, showing all the hidden costs of our not being able to work while we try not to die from COVID-19. I can see the point of the arguments, but the problem is, they won’t completely be solved by going back to work. Most of the problems “below the water”—suicide due to lack of income and stress, drug addiction, violence, non-COVID health problems being ignored because we can’t get to the doctor—will still be there once we go back to work and start getting sick faster.
Is someone more or less likely to turn to drugs, or suicide, if they lose their job because of a COVID-19 layoff, or because their life partner got sick for 30 days and got fired? Are young adults more or less prone to violence if they can’t get a job because of a stay-at-home order, or because they got sick and now have a significant cardiac problem, or lost a limb due to a blood clot?
The problem, as I understand it, is that we are discussing (that word again!) the difference between dying and working, and that’s not the crux. We are all going to get COVID-19 until and unless we get a vaccine. It’s not going away. It’s not going to die out. That’s not what viruses do. They persist, and we are not going to isolate this thing into oblivion. It’s here to stay, like cholera and mosquitoes.
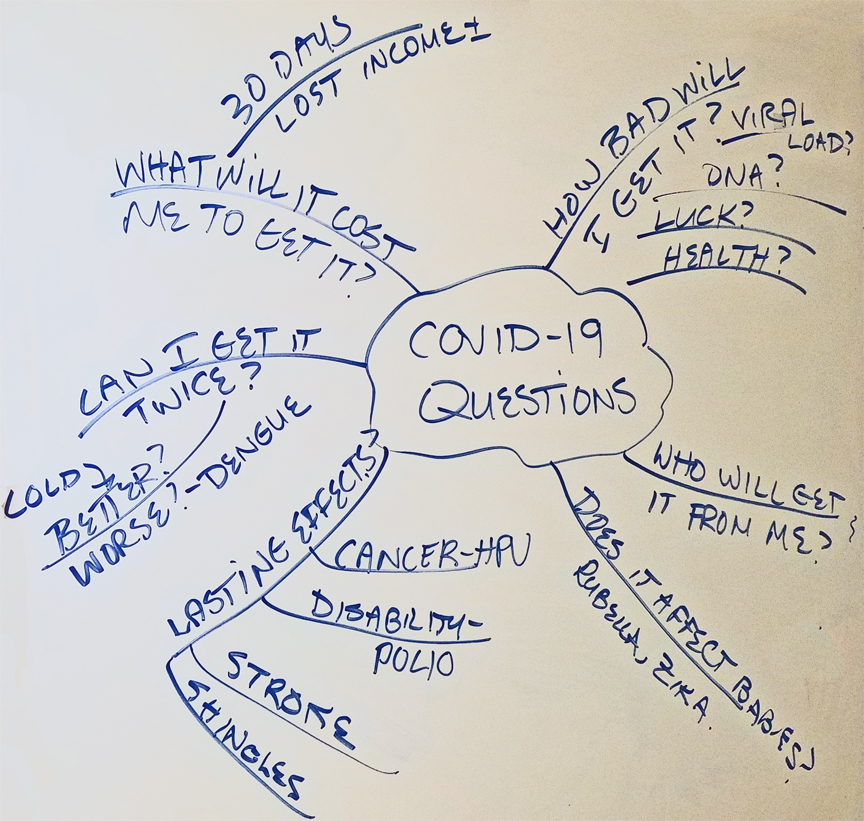
Mind map of COVID-19 questions
The questions I have cannot yet be answered. We don’t have this kind of data. In a few more months, we might.
How bad will I get it?
From a totally self-centered point of view, how sick will I—me, this instance, N=1, with MY risk factors, my health, my D3 levels, my (medication-controlled) BP, my Hg, my HbA1C, my lipid profile. Will I be barely inconvenienced, flat on my back for three weeks, or intubated? What are the variables that determine who gets knocked down and who doesn’t? We know one variable is viral load; we know others are co-morbidities. “Fat” is a co-morbidity, so nearly everyone I know is at risk. How fat is fat? Do I get points for having a high D3 and a low HbA1C?
It may turn out to be DNA-related, in which case I should get a 23andMe reading so I can get a warning when they figure that out.
Will I get it again?
Spare me the lecture on antibodies. The point here is, a) will I develop immunity at all, or b) is this virus immunity-proof, or c) will it mutate fast enough to invalidate any immunity (like HIV)? Dunno.
If I get it again, will it be better or worse than the first time?
We manage colds just fine. Some people get a milder case of dengue fever the first time, and then the second time, they come close to dying. Viruses have their own rules.
What will it cost me to get it?
This is a subset of “how bad”—for me, the cost is lost income because I’m a 1099 worker without sick leave. We have decent insurance, so most treatment-related costs will be covered.
Will getting COVID-19 leave lasting effects?
HPV causes cancer. Other viruses cause other cancers. Polio leaves people disabled, then comes back 40 years later and disables them again. Chickenpox comes back in the form of shingles. There are viruses in monkeys that can cause leukemia that kills other species of monkeys in five weeks. COVID-19 causes cardiomyopathy (ruined hearts) in some people that may lead to a need for a heart transplant in 10 years.
Will COVID-19 affect unborn babies?
Zika. Rubella. Enough said.
Who will get COVID-19 from me (besides my husband)?
Can I go to Thanksgiving and see my parents?
None of these questions shift the work/stay home discussion much at all. They are questions that everyone will face, whether we are staying home or going out in public. When the definition of “vulnerable” is opened up broader than “live or die,” it is obvious that we cannot shelter “vulnerable people,” because we do not know who is vulnerable.
Save this here for classifying the category on this post.

Follow Us!